
Region: Abdomen & Pelvis
List of Anomalies:
• Portosystemic venous shunt
• Persistent umbilical vein
• Duplication of the gallbladder
• Hypoplasia of the colon
• Duplication of the uterine cervical canal
• Longitudinal vaginal septum
• Persistent hymen
• Cryptorchidism
• Hypospadias
• Diverticulum of the urinary bladder
• Supernumerary teats
Anomalies Commentary:
In the fetus, the umbilical blood passes directly through the liver within the ductus venosus. This allows rapid flow of placental blood to the fetal heart. After birth the umbilical vein and ductus venosus atrophy so there is no longer a significant shunt through the liver. Postnatally, the portal vein conveys blood to the liver which has numerous sinusoids to provide a large surface for blood to exchange with liver cells. The sinusoids are drained by hepatic veins which enter the caudal vena cava. This is an example of a portal system (Latin, porta = gate), blood passes through two capillary beds before returning to the heart: gastrointestinal capillaries —> portal vein —> liver sinusoids —> hepatic veins.
The portal vein drains from the intestines and through the liver which acts as a filter to remove nutrients for storage and toxic substances such as molecules that are toxic to the brain. A portosystemic shunt allows portal vein blood to bypass the liver and enter the systemic circulation without being filtered by the liver. As a result, toxic substances reach the brain and cause neurological signs. This is most often seen in dogs and is diagnosed radiographically by injection of contrast media into the portal vein through a laporotomy incision. A portosystemic shunt can result from combinations of a persistent ductus venosus or anomalous veins that connect the portal vein to the azygos vein or to the caudal vena cava.
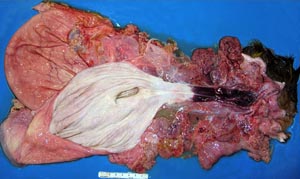
Male and female genital systems arise from two parallel duct systems. The mesonephoric duct system of males is derived from the ducts of the mesonephroric kidneys which are replaced by the definitive metanephoric kidneys. The paramesonephoric ducts of the female develop parallel to the mesonephoric ducts. Both ducts are present in the embryo but one duct system will atrophy as the other develops into the definitive genitalia according to the inherited genetic sex and resulting testicular hormones. Occasionally remnants of the opposite sex may persist or the paramesonephoric ducts may not fuse properly resulting in an anomaly.
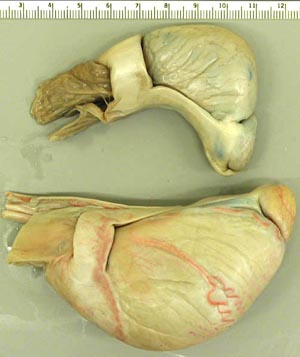
Cryptorchidism is the result of failure of testicular descent, the process by which the testicles descend from the abdomen into the scrotal sac. The gubernaculum testis pulls the testis to the inguinal canal; subsequently, elevated pressure pops the testis into the scrotal sac. The gubernaculum shortens due to pumping water out of its gelatinous matrix.
As descent of the testis occurs, the epididymis organizes and becomes closely associated with the testis proper so that the two are joined in the descended testicle. In abdominal cryptorchids there is less association between the testis and the epididymis but in inguinal cryptorchids the epididymis is closer related to the testis.
Testicular descent occurs to permit cooling of the testis. Cryptorchid testicles are small in size because at body temperature the germinal epithelium of the seminiferous tubules is reduced to a single layer. Body temperature does not affect growth of testosterone producing interstitial (Leydig) cells so a bilateral cryptochid stud will appear to be gelded but will have stud like behavior. Cooling of the testicle keeps the sperm inactive. They are activated by body temperature once delivered to the female genital tract. A high fever can elevate scrotal temperature enough to cause temporary infertility.
Anomaly Images:
Note: Click an image to see it enlarged, view its caption, and toggle its labels.
| 1 |  |
 |
2 |
| 3 |  |
 |
4 |
| 5 |  |
 |
6 |
| 7 | 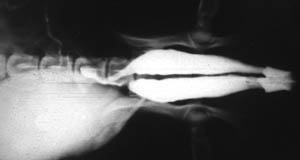 |
 |
8 |
| 9 |  |
 |
10 |
| 11 |  |
 |
12 |
| 13 |  |
 |
14 |
| 15 | 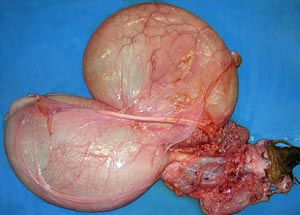 |
 |
16 |
| 17 |  |
 |
18 |